Editor’s Note: Kimberly Seals Allers (@iamKSealsAllers) is the founder of Irth App (@IrthApp) and executive director of Narrative Nation, a non-profit that creates technology and multimedia products to address racial disparities in maternal and infant health. She is the author of “The Big Letdown—How Medicine, Big Business and Feminism Undermine Breastfeeding.” The opinions expressed in this commentary are her own. View more opinion on CNN.
In 2020, Dr. Chaniece Wallace, a pediatrician who was a chief resident at Indiana University School of Medicine, died just two days after giving birth to a daughter, Charlotte.
Shamony Gibson studied at New York University and Medgar Evers College and died in 2019 just 13 days after giving birth to her second child.
In 2017, Dr. Shalon Irving, who was an epidemiologist with the US Centers for Disease Control and Prevention (CDC) and a lieutenant commander in the US Public Health Service Commissioned Corps, died three weeks after giving birth after being ignored when returning to the hospital for care.
In 2016 Kira Johnson, who had two degrees, spoke five languages and was the daughter-in-law of TV’s Judge Hatchett, bled to death after a routine C-Section in a Los Angeles hospital.

These tragic deaths highlight what Black women have known for years: that being well-educated and well-resourced simply are not fully protective factors when it comes to maternal mortality and morbidity. Serena Williams’s near-death experience after giving birth only underscored that.
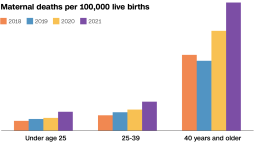
In 2020, Black women in the US were 2.9 times more likely to die during or after childbirth than white women, according to the US Centers for Disease Control and Prevention. More notably, a new study published in January showed that the wealthiest Black moms are more likely to die in childbirth than the poorest white moms. The study uses California administrative data to show how household income alone is not protective from racism’s impact on maternal and infant health outcomes. It is clear Black maternal mortality is not just a low-income problem.
But a current wave of policy and advocacy work is primarily focused on reimbursing doulas and offering needed pregnancy-related services to Medicaid-eligible patients. Doulas, trained birth professionals who serve as educators and advocates to pregnant women, have been shown to be both protective, improving birth outcomes for Black women, but also cost-effective by reducing the hospital expense of preterm births and C-sections.
In Oakland, the innovative Beloved Birth centering program with remarkable outcomes in reducing pre-term birth rates provides a doula, fitness trainer, chef-prepared meals for six weeks postpartum, a pregnancy photo shoot, midwifery-led prenatal visits, and a lactation consultant—but this comprehensive program is currently only available to Black women on Medical, the state’s Medicaid program. In New York City, the first free doula program is focused on marginalized zip codes.
“Just because you are not Medicaid eligible does not mean you can fully afford a doula or any other birth professional that Black women need,” said Tracie Collins, CEO and Founder of the National Black Doula Association (NBDA) and host of the Healthy Girl podcast in an interview via email. “Too many Black women are falling in the gap.”
Doulas are only one piece of a complicated puzzle that ultimately must include cultural change within medical institutions and systemic change overall. For years, much of the research into the rising Black maternal mortality rates treated Black women problematically – conflating income, education, and not getting prenatal care with high rates of preterm birth, low birthweight and maternal deaths.
Now there is more research reflecting the underlying reality that regardless of educational attainment or related factors like income, Black women experience higher maternal mortality rates across the board. So why aren’t more policy and advocacy efforts focused on providing pregnancy and postpartum services for Black women across the economic spectrum?
The misconception and narrative that Black maternal mortality rates are tied to income has already caused harm. Black women professionals, scientists and medical doctors have shared with me their near-death misses in childbirth; several of them also shared that they too considered themselves not at a high risk. “Many Black birthing folks reasoned ‘If the so-called research said the problem is being poor and unable to advocate for yourself and I’m not poor and am educated enough to advocate for myself then I will be ok,’ that’s false and dangerous thinking,” said Chanel Porchia-Albert, the founder and executive director of Ancient Song Doula Services, a Brooklyn-based organization that provides doula services to women of color and marginalized communities.
In my travels advocating for Black and brown patient experience data as a critical tool for systemic change, I meet many middle-class Black women who are not Medicaid eligible but don’t make enough to afford the costs of a doula or at-home postpartum support. Some ask friends and family to chip in and I encourage them to put it on their baby registry as something others can contribute to. But the idea of burdening other family and friends often does not sit well with them, and not every community member thinks of a doula as necessary when a crib, diapers and other essentials are also needed.

To be clear, efforts that focus on the needs of the under-resourced are critical. More than 3.3 million Black women,
or one in four nationally, are covered by Medicaid. According to the National Health Law Program’s Doula Medicaid Project, 11 state Medicaid programs currently reimburse doulas to a modest degree, and nearly a dozen are in some phase of the process to do so. This is an overdue recognition of the value of doulas and critical momentum to make sure they are accessible and paid a living wage.
But Medicaid coverage alone is insufficient to meaningfully address the nation’s Black maternal mortality crisis. This approach is short-sighted and continues to promote a dangerous narrative that research and too much anecdotal evidence has already disproven. “Medicaid covers the majority of births in our community and other payers often follow Medicaid’s lead when it comes to improving payment and coverage so setting the tone within Medicaid makes sense, but it can’t be the end goal,” Dr. Nathan Chomilo, Medical Director for Minnesota’s Medicaid & MinnesotaCare program, told me.
To improve the support Black birthing people receive, more commercial health plans should commit to reimbursing doulas as well. In Massachusetts, both the state Medicaid program known as MassHealth and private health plans are compelled to pay doulas who have met specified training and credentialing criteria.
Employers also need to step up and are positioned to provide access more directly. “Sixty five percent of people who get health insurance from their employer are in a self-funded plan – meaning those employers have a direct financial stake, in addition to the personnel/workforce stake, in keeping employees, including Black women healthy,” Chomilo told me.
The NBDA spearheaded a landmark partnership with Wal-Mart, one of the largest payers for pregnancy-related healthcare in the nation, to offer
doula services as an employee benefit.
Policymakers are paying long overdue attention to reducing high rates of mortality and morbidity among Black women. But they must go further to fully address the maternal mortality disparities by addressing racism and bias in care beyond mandating training for healthcare providers without accountability, pushing for cultural and systemic change within medical schools and health systems, funding midwifery care models and birth centers for low-risk pregnancies, and ensuring there is policy advocacy and change across the economic spectrum for Black women.
“We are all at risk when we choose to see the issue of Black maternal health from one side,” said Porchia-Albert.
In practice, principle, research, advocacy and messaging, we must leave no Black woman behind.